
This page gives information on ACL tears. To know more about Arthroscopic ACL reconstruction surgery click here
What is Anterior Cruciate Ligament(ACL)?
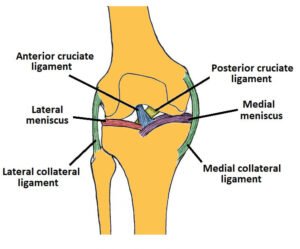
The anterior cruciate ligament (ACL) isone of the four main ligaments in the knee. It is a strong band of dense connective tissue that connects the thighbone (femur) to the shinbone (tibia), runningdiagonally through the middle of the knee.
What is the function of ACL?
- Stabilizes the knee joint by preventing the tibia from sliding forward in front of the femur.
- Limits rotational movements of the knee
- Contributes to overall joint stability, mainly during activities involving stopping, turning, jumping, pivoting or other dynamic movements.
- Without a functioning ACL, the knee often becomes unstable, particularly during movements that require rapid changes in direction or pivoting.
How does ACL rupture or tear happen?
The ACL is the most commonly injured ligament in the knee. An ACL rupture or tear happens when the knee is subjected to forces that exceed the ligament’s capacity, often during activities involving sudden stops, rapid changes in direction, twisting, pivoting, or awkward landings from a jump. These can happen in sports like basketball, football, kabaddi or during road traffic accidents.
Who is more prone for ACL injuries?
People who are more prone to ACL tears typically have one or more of the following characteristics:
Female sex:
Women are about three times more likely to suffer ACL injuries than men. This increased risk is linked to anatomical differences, hormonal influences, greater ligament laxity, and neuromuscular factors like landing mechanics.
Participation in high-risk sports:
Sports that involve frequent pivoting, sudden stops, jumping, or rapid changes in direction—such as soccer, basketball, football, volleyball, skiing, tennis, kabaddi—carry a higher risk.
Previous ACL injury:
People who have had a previous ACL tear or reconstruction are at higher risk for another ACL injury, either in the same or the opposite knee.
Anatomical factors:
Certain knee and lower limb shapes, such as a narrow femoral intercondylar notch, increased tibial slope, shallow medial tibial plateau, and greater Q angle, can increase risk.
Neuromuscular and biomechanical factors:
Poor proprioception, weak core or hip muscles, imbalanced strength between quadriceps and hamstrings, faulty landing mechanics, and dynamic knee valgus are risk factors, especially in young athletes.
Age(most common between 15 and 45 years) and high body mass index (BMI) may also contribute to increased risk.
What are the symptoms of ACL injury?
- A loud pop or popping sensation in the knee at the time of injury.
- Severe knee pain, especially when trying to bear weight or move the joint.
- Rapid swelling of the knee, usually developing within the first 6 to 24 hours.
- Feeling of instability or the knee “giving way”, particularly during weight-bearing activities or changes in direction.
- Loss of full range of motion in the knee.
- Difficulty continuing activity or inability to keep playing sports after the injury
What is the immediate management following a knee injury?
The immediate management of knee injuries focuses on minimizing pain, swelling, and further damage. These include:
- Protection: Remove the person from play or activity to prevent further injury.
- Rest: Avoid activities that cause pain and offload the knee as much as possible. Crutches may be used if weight-bearing is painful.
- Ice: Apply an ice pack to the injured area for 15–20 minutes every 1–2 hours while awake, for the first 48–72 hours. Do not apply ice directly to the skin to avoid burns.
- Compression: Use an elastic bandage to wrap the knee, starting below and finishing above the joint. The bandage should be snug but not so tight that it restricts blood flow.
- Elevation: Keep the knee elevated as much as possible, especially in the first 24–48 hours, to reduce swelling.
- Medical Care: Visit your nearest medical services for further evaluation and management.
What are the investigations needed?
- X-rays (Radiographs): Used to rule out fractures, assess joint space. ACL tears cannot be diagnosed with radiographs. Only indirect signs can be identified (Eg. Segond fracture, bone bruise, lipohaemarthrosis)
- MRI (Magnetic Resonance Imaging): Gold standard imaging for ACL injuries, with accuracy of 95% or better. MRI also detects associated meniscal tears, chondral injuries, bone bruises, and other soft tissue damage.
What are the treatment options for ACL tears?
ACL management should have an individualized approach. Both operative and non-operative treatments are acceptable. Multiple factors are considered when deciding on ACL management, including the patient’s age and demands, activity level, sports participation, and the injury status of other supporting and stabilizing structures.
Non-operative management:
This is indicated where there is reduced ACL laxity in low-demand older patients. These patients are usually managed with physiotherapy and lifestyle modifications. Non-operative treatment is indicated in partial ACL tears as well.
Arthroscopic ACL reconstruction:
This is indicated in a complete ACL rupture in younger active or older active high-demand patients. The primary objective is an anatomical ACL reconstruction to reinstitute the stability of the knee, consequently reducing the chances of secondary meniscal or chondral injuries. To know more about the surgery Click here