
This page gives information on the surgical management of Anterior cruciate ligament injuries. To know more about ACL tears in general, Click Here
When do I need this surgery?
Arthroscopic reconstruction of ACL is needed if you have one or more of the following indications:
- Symptomatic knee instability: Recurrent episodes of the knee giving way during daily activities or sports.
- Desire to return to pivoting or high-risk sports
- Young age and high activity level
- Associated injuries: Presence of additional intra-articular damage such as meniscal tears or significant anterior tibial subluxation.
- Failure of conservative management: Persistent symptoms despite appropriate non-surgical treatment, such as physiotherapy.
- Chronic ACL injury with instability: Long-standing tears with ongoing instability or functional limitations.
What are the benefits of the surgery?
The main aim of ACL reconstruction is to restore knee stability, function, and prevent further joint damage, especially in active individuals. After surgery your knee should not give way anymore. This will allow you to be more active and you may be able to return to some of or all your sporting activities.
What will happen if I don’t have surgery?
Athletes do not usually do well without surgery. If you are someone with very active lifestyle and are involved in recreational sports activities/gym/running you are more likely to have instability (buckling or giving away). Frequent buckling of knee can lead to more cartilage damage and early arthritis. If your knee continues to give way, you can get a torn meniscus (risk: 1 in 30).
What does the surgery involve?
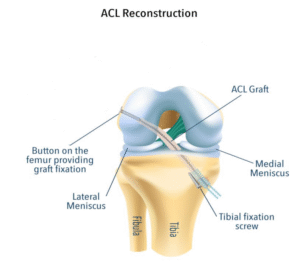
This is a key hole surgery (arthroscopy). The procedure involves reconstructing your ACL with your own tendons. You will be given antibiotics during the operation to reduce the risk of infection. The operation usually takes 60 to 90 minutes. One or more cuts are made around your knee. The tendons are harvested from inner side of the knee and used as graft. Drill holes (tunnels) are made into the bones (femur and tibia) and the graft is fixed to the tunnels using special anchors and biodegradable screws. The skin is closed with sutures or clips.
What are the grafts that can be used for the reconstruction?
The 3 main grafts used for ACL reconstruction are the following
- Hamstring tendon autograft: Usually uses the semitendinosus and gracilis tendons. Most commonly used.
- Quadriceps tendon autograft: Harvested from the central quadriceps tendon, sometimes with a bone block from the patella.
- Bone–patellar tendon–bone (BPTB) autograft: Uses the middle third of the patellar tendon with bone plugs from the knee cap and tibia.
What is the usual outcome of this surgery?
Knee Stability:
95% of patients have stable knees 15–20 years after surgery, with significantly less instability compared to non-surgically treated patients.
Patient Satisfaction:
The majority of patients report being “very satisfied” or “satisfied” with their surgical outcome, and a large proportion (often over 85%) return to their pre-injury activity level.
Quality of Life:
Quality-of-life scores (e.g., KOOS) improve markedly after surgery, reflecting better knee function and reduced symptoms.
Arthroscopic ACL reconstruction is highly effective in restoring knee stability and function, enabling most patients to return to normal activities and sports, with sustained benefits over the long term
What are the complications that can happen?
- Bleeding during or after the operation (risk: 1 in 25): Usually this settles with rest and ice fomentation.
- Infection: The risk is <1% in key-hole surgeries. Most infections can be managed with a course of antibiotics. Rarely surgery is needed to wash out the knees.
- Damage to nerves around your knee, leading to weakness, numbness (risk: 1 in 300). This usually gets better in a few months’ time.
- Loss of knee movement, preventing full bending (<2%) or straightening (<1%). This usually improves with physiotherapy.
- Your knee keeps giving way, if the ligament graft fails caused by it gradually stretching or a further sports injury (risk 5%).
What is the usual timeline and recovery after this surgery?
- Length of hospital stay: 1-3 days
- Total recovery period: 6 months
- Return to driving: 6-8 weeks
- Return to sports: 6-9 months
- Return to work: Desk based job – 2-3 weeks
Manual job – from 3 months